DISEASE INFO
What is influenza?
Equine influenza is a highly contagious respiratory disease of horses and other equidae, including donkeys and ponies. Equine influenza was first discovered in 1963 and since then has become endemic in many countries. In fact, the spread of equine influenza has been so rapid that today very few countries are free from infection. Currently New Zealand and Iceland hold a disease-free status. However due to the nature of the disease and the global transport of horses, these countries remain at high risk of introduction of disease if quarantine measures fail. While it does not usually cause a long term or fatal illness, a horse will be unwell and require time off exercise sometimes for an extended period.
Epidemiology (Factors influencing occurrence of disease):
Influenza A viruses infect many different species such as humans, horses, swine and birds. Wild birds play an important role in the worldwide spread of influenza viruses and transmission of influenza has been demonstrated between wild birds and horses.
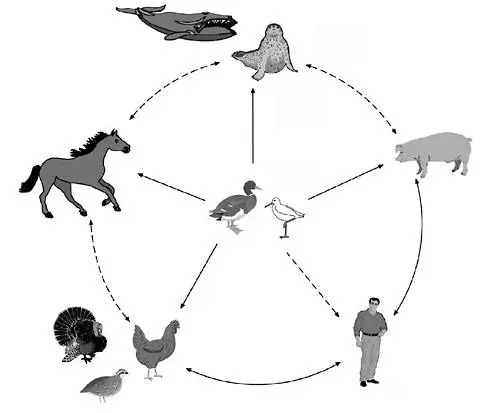
Images from: The Threat of Pandemic Influenza: Are We Ready? Workshop Summary ( 2005 )
Influenza is an airborne virus and can spread quickly and easily through a yard. Under favourable weather conditions it can spread up to 5km. It can be transmitted by direct horse-to-horse contact and also via people, tack, feed and equipment. Disease can lead to serious complications in very young or old horses and due to its infectious nature can spread rapidly through groups of unprotected animals.
Equine influenza, like other influenza viruses, undergoes continuous antigenic change. Antigenic drift and antigenic shift may help the virus elude an immune system that has been previously primed by vaccination or natural exposure, leading to outbreaks of disease among supposedly protected horse populations.
Transmission occurs by inhalation of respiratory secretions, most commonly via nose-to-nose contact and can spread quickly and easily through a yard. However, the virus can be windborne. Aerogenous transfer of virus has been confirmed over distances of 1 to 8 km, depending on the climate and prevailing weather conditions. Fomites such as tack, grooming equipment, machinery, water, feed, human contact and perhaps also flies play a role in transmission. The virus does not survive well in the environment however and can easily be killed by heat, cold, desiccation, and disinfectants.
Shedding of the virus in nasal secretions begins as soon as 24 hours after infection and shedding can continue for 7 to 10 days in some horses.
Infection may occur within any age group, breed, sex, and season. However, poorly ventilated, indoor housing is a risk factor in the development of outbreaks of disease.
Indoor housing places the horses in closer contact and facilitates the transmission of disease. Virus spread is particularly pronounced in racing yards, where large numbers of young horses congregate (1-5 year old). Young immunologically inexperienced horses and unvaccinated horses are particularly susceptible.
There are a range of different clinical outcomes following influenza virus infection, depending on the infecting virus, its virulence and level of exposure as well as innate host defences and the immune status of the host. The immune status of the host is also influenced by a number of factors including vaccination status, time since last vaccination, stress, age, exercise and secondary infection. Vaccinated horses generally develop few or no clinical signs following infection but they can pose a risk to other (non-vaccinated) horses as a result of virus excretion after challenge from field virus, albeit a lower risk than the field infection itself.
The disease is characterised by high morbidity (almost 100% in some populations) and low mortality. Occasional fatalities may occur in debilitated horses, donkeys and following infection with some secondary bacterial invaders.
Clinical signs
Clinical signs following infection vary greatly depending on the immune and health status of the infected equid. The incubation period for the virus is generally short (1-3 days). The earliest clinical signs of infection include; a rapid rise in body temperature (up to 106°F), depression, anorexia, clear nasal discharge, harsh dry cough and enlarged lymph nodes in the head and neck region. Increased inspiratory and expiratory sounds are often heard on auscultation of the chest. In uncomplicated cases these signs resolve within 2- 5 days. However, a lingering cough and secondary bacterial infection may delay the recovery for weeks to months. Secondary bacterial infection should be suspected in any case that persists beyond 5 days, with pyrexia and mucopurulent nasal discharge. Common complications recorded following influenza include; pneumonia, pleuropneumonia and bronchitis. Less commonly vasculitis, sore muscles and myocarditis (heart muscle inflammation which can subsequently cause an irregular heartbeat) have been reported. Occasionally rapidly fatal primary viral pneumonia occurs in young foals.
The severity of symptoms depends on numerous horse related factors such as age, stress, exercise level, vaccination status but also on how potent the infecting virus is. Naïve unvaccinated horses experiencing infection for the first time are likely to show marked signs whereas other horses may only show mild signs which can be easy to mistake for something else. However, the disease carries a low rate of mortality so it is unlikely that your horse will die from infection. However, the virus can cause a form of pneumonia which may prove to be fatal in foals or yearlings.
Partially immune (vaccinated or previously infected) horses may demonstrate mild or no clinical signs.
Diagnosis
Due to the rapid spread of the disease it is vital to diagnose equine influenza as early as possible. Usually the earliest diagnosis is based on suspect clinical signs in association with a suspected exposure to infection.
A more definitive diagnosis is based on virus isolation from nasopharyngeal swabs or paired serum samples. The first of two paired serum samples is collected as early in the disease course as possible (acute phase) and the second serum sample is collected 2 weeks later (convalescent phase). Virus isolation from nasopharyngeal swabs can also provide much needed information on the antigenic drift and shift of the virus. PCR testing may also be used to detect segments of the viral RNA from the nasopharyngeal swabs. This highly sensitive test is becoming more readily available.
Cytology and bacterial culture may be of interest if a secondary bacterial infection is suspected.
In general, sampling should be performed in early clinical cases to increase the success rate of the diagnostics.
Treatment and Control
Treatment for horses with influenza is largely based on supportive care. Horses that do not develop complications may simply require strict stall rest and high quality nutrition. A simple rule of thumb regarding the suggested length of the rest period is; 1 week of rest for each day of fever. If horses are returned to work too early then the likelihood of secondary complications is increased. A minimum period of 3 weeks rest must be observed.
Good nursing care, clean water, palatable food, and clean, dry, dust-free bedding should be made available. Electrolyte solutions may be provided in addition to clean plain water.
Nonsteroidal anti-inflammatory drugs (NSAIDs) may be administered in pyrexic animals but should be used with caution in dehydrated horses.
Antibiotics may be required if the horse is at risk of secondary bacterial infection or is demonstrating clinical signs (i.e. fever persisting beyond 3-4 days, mucopurulent nasal discharge or pneumonia).
Antiviral agents are of little use in horses already exhibiting clinical signs but your veterinary practitioner may prescribe these agents to protect valuable horses from infection during an outbreak. In-contacts may be treated prophylactically or treated based on a rise in body temperature, indicating early disease.
Prevention
Prevention of disease is based on a combination of hygienic management practices and vaccination.
Suggested management practices that reduce the exposure of horses to disease include:
- Adequate nutrition
- Stress reduction
- Isolated newly introduced horses for 2-3 weeks
- Separation of susceptible animals from horses prone to exposure (i.e. separate foals, mares, yearlings, geriatrics and immunosuppressed horses from performance horses that travel)
- Separate travelling horses from resident horse population if possible
- Surveillance of the herd for onset of clinical signs is vital
Vaccination
Vaccination of at-risk horses is vital for the individual animal and also to the control of the spread of disease within the equine population. High levels of vaccination coverage will reduce the susceptible population and help to reduce the significant economic losses equine influenza causes in the equine industry.
A variety of influenza vaccines are available on the market, under prescription control, either as single component vaccines or as combined influenza and tetanus vaccines . MSD Animal Health markets both options. The duration of immunity of vaccines is variable. It is advisable to consult the product SPC or your veterinary practitioner for advice on correct vaccination timing and regimes.

Equine influenza is a highly infectious respiratory disease of horses. Found almost worldwide, the disease will affect a worrying percentage of horses in their lifetime. Learn how you can do your part to protect against Equine influenza and keep the bonds strong.